Adjunct Clinical Professor in the Division of Environmental and Occupational Health Sciences and th INSPE Associates, Illinois
Background & Introduction: There are two principal data series tracking pediatric exposure to cannabinoids which have complementary strengths. One is the Pediatric Health Information System (PHIS) which is a database covering approximately 50 children's hospitals in the US. (1) The second is the National Poison Data System (NPDS) which is administered by America's Poison Centers and covers the entire population of the 50 United States, the District of Columbia, and all US territories. (2) Two recent studies with PHIS show sharp increases, as does the most recent but much older study with the second data series, NPDS. The purpose of this note is to provide an updated longitudinal report based on the NPDS data.
Methods: In 2000, the NPDS Annual Report had one category for marijuana (the term they used). As more marijuana products have become available, that category has been subdivided, with the overall rubric renamed “cannabinoids and analogs.” In the most recent NPDS Annual Report (2023), there were 17 subcategories of cannabinoids and analogs, categories which including marijuana: concentrated extracts, marijuana: dried plant, and marijuana: edible preparations.
Using the NPDS Annual Reports for each year, the number of exposures of children under 6 years of age reported to NPDS was tabulated. NPDS began tracking the 6-12 age group in 2009. The number of reported exposures for the 6–12 group was tabulated for each year from 2009 to 2023.
The subcategory of marijuana: edible preparations was added to the NPDS Annual Report in 2016. For both the under 6 and the 6-12 groups, annual numbers of reported exposures to edible marijuana preparations were tabulated from 2016 through 2023.
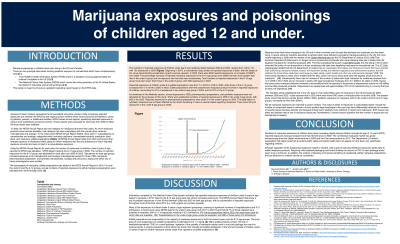
Results: The numbers of reported exposures of children under age 6 was relatively stable between 2000 and 2009, ranging from 108 to 141, with 132 exposures in 2009. Beginning in 2010, a consistently rising number of reported exposures is seen, with the shape of the curve demonstrating acceleration (graph of data concave upward). In 2023, there were 8400 reported exposures, an increase of 6363% from 2009. The percentage increase of reported marijuana exposures in the 6-12 age group since 2009 has been even greater than that of the under 6 group and that number has also been accelerating, though numbers of reported exposures in the 6-12 age group have been lower than those in the under-6 group, with 3023 exposures in 2023.
Reported exposures of children under 6 to edible preparations rose from 7 in 2016 to 4795 in 2023, while those in the 6-12 group increased from 0 in 2016 to 2025 in 2023. Edible preparations were the predominant marijuana product involved in reported exposures of children, accounting for 57% of exposures in the under-6 age group in 2023, and for 67% in the 6-12 group.
Conclusion & Discussion: Exposures of children under 6 and 6--12 have increased by >6000% since 2009. Edible preparations cause the majority of marijuana exposures in both age groups. The toxic dose of edible marijuana in pediatric populations is estimated to be 1.7 mg/kg. Ingestion of the quantity of marijuana found in one package can result in serious toxicity. A recent study has shown that virtually all hospital admissions of children under 10 years of age for severe marijuana toxicity result from ingestions of edible preparations.
Limitations: NPDS Annual Reports do not include data that allow outcomes for specific age groups to be determined. Demographic data other than age are not available in the Annual Reports. Other studies referred to in this poster must be used to understand those aspects of this topic. Additionally, not all marijuana exposures are reported to poison control centers.
Conclusion: Stronger regulation of the marijuana market is needed to reduce childhood exposures particularly to edible marijuana products. Requiring child-resistant packaging and further limiting the amount of THC in each package would seem to be a minimum expected response. In addition, the wisdom of allowing commercial marketing of sweetened, edible marijuana preparations that are attractive to children should be considered.
References: 1. Bennett CE, Venkataramani A, Henretig FM, Faerber J, Song L, Wood JN. Recent Trends in Marijuana-Related Hospital Encounters in Young Children. Acad Pediatr. 2022 May-Jun;22(4):592-597. doi: 10.1016/j.acap.2021.07.018. Epub 2021 Jul 26. PMID: 34325061. 2. Walsh PS, Dupont AS, Lipshaw MJ, Visotcky A, Thomas DG. Cannabis Legalization and Resource Use for Ingestions by Young Children. Pediatrics. 2024 Jun 1;153(6):e2024065881. doi: 10.1542/peds.2024-065881. PMID: 38690624; PMCID: PMC11153323. 3. Onders B, Casavant MJ, Spiller HA, Chounthirath T, Smith GA. Marijuana Exposure Among Children Younger Than Six Years in the United States. Clin Pediatr (Phila). 2016 May;55(5):428-36. doi: 10.1177/0009922815589912. Epub 2015 Jun 7. PMID: 26054783. 4. Pepin LC, Simon MW, Banerji S, Leonard J, Hoyte CO, Wang GS. Toxic Tetrahydrocannabinol (THC) Dose in Pediatric Cannabis Edible Ingestions. Pediatrics. 2023 Sep 1;152(3):e2023061374. doi:10.1542/peds.2023-061374. PMID: 37635689. 5. Cohen N, Mathew M, Brent J, Wax P, Davis AL, Obilom C, Burns MM, Canning J, Baumgartner K, Koons AL, Wiegand TJ, Judge B, Hoyte C, Chenoweth JA, Froberg B, Farrar H, Carey JL, Hendrickson RG, Hodgman M, Caravati EM, Christian MR, Wolk BJ, Seifert SA, Bentur Y, Levine M, Farrugia LA, Vearrier D, Minns AB, Kennedy JM, Kirschner RI, Aldy K, Schuh S, Campleman S, Li S, Myran DT, Feng L, Freedman SB, Finkelstein Y. Severe outcomes following pediatric cannabis intoxication: a prospective cohort study of an international toxicology surveillance registry. Clin Toxicol (Phila). 2023 Aug;61(8):591-598. doi: 10.1080/15563650.2023.2238121. Epubm2023 Aug 21. PMID: 37603042
Learning Objectives:
describe what has happened with pediatric exposures of children 12 or under to marijuana since the year 2000.
verbalize what is the main marijuana preparation involved in the exposures.
describe the known medical consequences of pediatric exposures to marijuana.